CrossFit elbow injuries
|

This article is for information purposes only and in no case replaces the assessment and prescription of an individualized treatment by a health professional.
The elbow is one of the main joints in Crossfit sports practice, as it is responsible for transmitting loads through the arm and stabilizing.
Although it is not one of the most damaged areas of the body, as the shoulder, knee and lower back are the most frequently injured, the elbow deserves special attention.
Affecting 3-6% of Crossfit athletes, the elbow is a joint involved in both gymnastic and weightlifting movements, from the simplest to the most complex. Therefore, an injury to this joint can be disabling for the athlete.
Factors such as joint hyperlaxity, poor technique or inadequate progression of loads increase the risk of injuries such as tendinopathies, instabilities or overuse overloads.
Anatomy of the elbow joint
The joint is made up of three distinct bones, which are the humerus, the ulna and the radio.
Within the types of joints, the elbow is called a synovial joint or diarthrosis, since we have two distinct joints within the elbow complex, the humero-ulnar joint and the humero-radial joint.
In this type of joint, the bones are separated from each other by a thin layer of hyaline cartilage and their movements are lubricated thanks to the synovial fluid inside the joint capsule covered by the synovial membrane.
As for the ligaments that we can find in the elbow joint limiting and stabilizing the movements we can find:

The elbow musculature crosses the joint thus improving the stability of the joint by working as active stabilizers.
We can find:
- Muscles that perform elbow flexion:
- Biceps brachii.
- Brachioradialis.
- Anterior brachial.
- Muscles that perform elbow extension:
- Triceps brachii.
- Anconeo.
- Muscles involved in supination of the forearm:
- Biceps brachii.
- Short supinator.
- Muscles involved in forearm pronation:
- Round pronator
- Square pronator
- Long palm
- Radial carpal flexor
- Medial musculatureinsertion in medial epicondyle of the humerus: mainly involved in wrist and finger flexion and ulnar and radial deviations.
- Round pronator
- Radial carpal flexor
- Ulnar flexor carpi ulnaris
- Long palm
- Superficial flexor of the fingers
- Lateral musculatureinsertion in lateral epicondyle of the humerus: extension of wrist and fingers
- Radial extensor carpi radialis brevis
- Finger extensor
- Little finger extensor
- Ulnar extensor of the carpus
- Supinator
- Anconeo
Biomechanics of the elbow
In the elbow we can find three different joints:
The normal range of motion of the elbow is from 0° in extension to 140° in maximum elbow flexion.
Within which, we can find ranges of elbow hyperextension due to ligament and joint hyperlaxity that some people have.
In daily life, movements range from 30º to approximately 130º.
The humero-radial joint allows 180º of pronation-supination, being necessary for daily life 50º of supination and another 50º of pronation.
Context in CrossFit
Weightlifting movements
In movements such as the snatch and overhead squat, we find that the elbow must remain in a locked position in extension and slight supination to keep the bar overhead.
Here comes into play a co-contraction of triceps, pronator, supinator and forearm musculature to generate the necessary stability, because if there is hyperlaxity or motor control is not adequate, there may be an excess of valgus, compromising the integrity of the medial collateral ligament.

On the other hand, in jerk movements, the elbow goes from sub-maximal flexion to full extension in a very short period of time, which makes it the lock must be strong and stable.
The structures involved in this gesture must be prepared for such a rapid change, otherwise it may result in the blocking not being performed correctly due to fatigue or technique, which puts the joint at risk.
Gymnastic barbell movements
In this type of exercise the elbow must be maintained and controlled throughout the movement with good stability against eccentric forces, as for example in kipping movements there are very sharp drops or muscle-ups.

In fact, in this exercise the elbow is stressed by the step it has to make in the transition phase, as it changes from doing the pull-up to a powerful extension.
The elbow connects the work of the trunk and shoulder with that of the forearm and wrist/hand, therefore, in kipping movements, you must control the changes of direction without losing alignment, otherwise, the decompensation of forces can be greater, generating instability.
Pushing gymnastic movements (HSPU, HSW...)
A powerful extension of the elbow is performed, mainly by triceps and anconeus.
You must have a very powerful stability, since being in inverted position, we are carrying all the weight of the body and it is who controls the movement as well, receiving all the axial load in a direct way.

Co-contraction of triceps and flexor and extensor muscles of the forearm.
Most common elbow injuries
Lateral epicondylalgia
It is an affectation of the tendon of the musculature of the extensor group, of the epicondylar muscles, since its tendon is the one that reaches the lateral epicondyle of the humerus. The main muscle that is usually affected is the extensor carpi radialis brevis.

Among its symptoms we can find pain in the lateral aspect of the elbowThis is not always the case, but may also be accompanied by pain in the dorsal aspect of the forearm.
This pain usually worsens with gripping, as well as weight lifting or repetitive movements of the forearm. There may also be weakness when making manual grasping gestures as the pain itself is inhibitory.
This type of injury is the most frequent in Crossfit due to the high intensity training and the amount of gripping exercises during the activity, whether it is gymnastics, weightlifting, dumbbells or Kettlebell, we are using the grip, so it is easy to generate an injury. overload in the area for not being well adapted to so much training volumeIf we do not generate adequate rest, we will be giving a constant stimulus to the area.
This will increase fatigue thus facilitating possible injury.
Also a poor traction pattern can generate this injury, being affected in basic traction exercises such as pull-ups, but also in the pulling phase of weightlifting exercises, which can generate muscular imbalance between the supinator and pronator musculature of the forearm with a deficit in eccentric control when doing butterfly movements mainly.
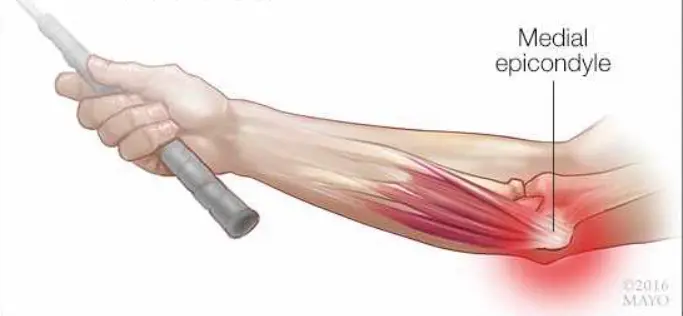
Medial epicondylalgia
Injury that causes pain in the medial aspect of the elbow, in the medial epicondyle of the humerus, since this is the origin of the epitrochlear muscles, which are those that perform wrist flexion and forearm pronation. Normally the most affected muscles are the radial carpal flexor and pronator teres.
This lesion presents with fingertip pain in the medial epicondyle of the humerus, generating pain when flexing the wrist or pronating the forearm, mainly against resistance, although if the pain is of long evolution, it may appear earlier with less resistance radiating towards the forearm.
Among its most frequent causes, we can find intense or maintained grips, as well as a lot of exercise with the wrist in extension, such as very heavy front squats or heavy cleans with poor reception.
Athletes who have less polished technique in gymnastics or who have excessively high volume are most likely to suffer from this injury, as well as those with elbow hyperlaxity.
Tendinopathy of the biceps or triceps brachii
The distal biceps brachii tendinopathy gives pain in the anterior aspect of the elbow, being painful the movements of elbow flexion or resisted forearm supination.
It presents pain mainly when doing gymnastic exercises such as pull-ups or when lowering during the execution of muscle-ups.
Weakness or a feeling of tension in the anterior aspect of the elbow may appear.
This injury can occur due to supination overload such as when performing many rope climbs or chin-ups, uncontrolled eccentric loading when doing muscle-ups both on rings and barbell, technical failure due to elbow hyperextension and an imbalance between shoulder and scapula due to lack of proximal control.
The triceps tendinopathy presents with pain in the posterior aspect of the elbow in gestures such as resisted elbow extension.
There is usually pain or discomfort in both vertical and horizontal thrusts, and there may be a speed deficit when performing the elbow lock in exercises such as the snatch or jerk.
It can appear due to an excessive volume of pushing exercises such as HSPU, muscle-ups, bench press, dips, strict press... also due to that fatigue generated by repetition in blocking exercises or bad technique, as well as repeated hyperextension with load or poor eccentric control in these exercises without good triceps activation.

Olecranian bursitis
The bursa is a type of pad that serves as a lubricant between the joint and the soft tissues of the elbow, if inflamed it can cause swelling, pain and redness.
It is not very common in Crossfit, but can be caused by repetitive microtrauma or direct trauma to the area after a fall.
The pain is usually mechanical, i.e., when resting on the affected area or rubbing.

Biomechanical and technical factors related to elbow injuries in CrossFit.
Joint hyperlaxity
Joint hyperlaxity is one of the main risk factors for elbow injuries, as it can lead to both acute and chronic injuries of the elbow itself.
It is a condition in which joint capsule and ligaments are more elastic than normal, which allows greater range of motion than usual, since they do not act as a brake on movement as they should.
An athlete may have global or local hyperlaxity at the elbow, resulting in a greater reliance on muscular and neuromotor control to generate this stability.
What risks can we find associated with hyperlaxity in CrossFit?
- Joint dislocation or subluxation, especially when we have direct load on the joint, HSPU, HSW...
- Ligament injuries, mainly due to excessive valgus or varus in bad receptions when snatching.
- Functional instability, since the non-contractile structures do not act adequately to stabilize the joint through motor and muscular control.
It is important for this type of athlete to learn to perform elbow extension in exercises such as the snatch or jerk without generating that passive blockage generating hyperextension of the elbow, since repetition and fatigue of the adjacent structures, which are controlling less and less, can cause damage to the elbow.
For that, it is important that they frequently perform personalized training with exercises to work on motor control and elbow stability. In addition to avoid working joint mobility in extreme ranges, because if an athlete has excess mobility and continues to work it in excess, it can generate more instability.
Compensation for shoulder and/or wrist mobility deficits
Among the most common limitations in the shoulders, we can find both limitation in flexion and external rotation mobility, as well as deficits in muscle activation to generate scapular stabilization.
Therefore, in the overhead movementswhen adequate mobility is not reached to generate this movement, the elbow will be required to over-act by over-activating in order to stabilize the bar and prevent it from falling forward, as well as in the pull-ups, if the scapular activation is not adequate, the activation of the biceps brachii and brachioradialis will be much greater and can generate overload in that musculature.
In the wrist, there is usually a deficit of mobility in extension and a lack of mobility in prone/supination.
This means that in front rack movements, since we do not have this extension, we have to raise the elbow more, generating more tension in the elbow flexor muscles.
Also in HSPU or HSW exercises, if we do not have adequate extension, a more active control by the elbow stability will be generated, which can lead to fatigue in the musculature generating varus or valgus destabilizations.
Role of motor control and proprioception
The motor control is defined as the ability of the nervous system to organize and execute precise, efficient and safe movements.
The proprioception is the ability to perceive a position in space without the need to be looking at it.
Both capabilities are of utmost importance for the recovery of an elbow injury, as it will involve a lot of conscious work of that area.
In injuries mainly, as we have seen, of instability, there is an alteration in the contraction pattern, which affects the active stabilization of the elbow, generating muscular decompensations and differences in the contraction patterns when performing certain complex movements such as a push jerk.
This results in a disorganization of muscle activation during exercise, causing loss of joint protection reflexes, which increases the risk of injury, especially in patients with hyperlaxity.
In fact, these skills should be worked on from the early stages in order to avoid possible relapses and to have a functional and stable elbow, avoiding instability and hyperextension patterns.
Thus, exercises are generated from the base, to activate the muscles that may have been affected in the injury, evolving to more complex tasks by introducing exercises with high cognitive demands, increasing speed and resembling CrossFit exercises so that when the athlete returns to perform wods again, he/she will have no problem performing the exercises that demand the most from him/her.
Suggested exercises
The following exercises will be proposed for the recovery of elbow pain.
As general rules always avoid full hyperextension of the elbow so that stability is actively worked. by the musculature.
As for the exercises, we move towards more complex progressions of the same. This allows the stimulus to evolve and progress in order to recover the functionality of the elbow.
1. Rubberized forearm supination
To do this exercise, it is important to have the elbow next to the ribs. Once the forearm is in 90º flexion and perpendicular to the rubber (which is in tension) proceed to rotate the forearm in a controlled manner until the palm of the hand is facing upwards, controlling the turn, so that the rubber does not pull the forearm abruptly.
2. Forearm pronation with rubber
As in the previous exercise, the elbow should be next to the ribs, to avoid compensations. Once the elbow is in this position, we will perform the counter-resistance pronation with the elastic band. Once the elbow is in its maximum pronation, the eccentric part of the exercise will be performed in a controlled manner.
3. Prone-supination with pike
In this exercise, the elbow should be next to the ribs. The gesture of rotating the forearm should be performed in a slow and controlled manner, in order to work the muscles.
4. Farmer carry unilateral
When picking up the kb, full hyperextension of the elbow should be avoided, otherwise the elbow musculature will not be working. To work on its stability, a semi-flexion of the elbow should be performed. In addition, by doing the exercise unilaterally, we will be working on the stabilization of the shoulder.
5. Slow tempo triceps dips on the box
With the hands on the box, positioned with the same opening as the shoulders, an elbow flexion with controlled shoulder extension will be performed to work the triceps.
6. Isometric bending
When performing this exercise, try to stay in a push-up position. Progress in terms of longer time and greater elbow flexion, as the pain subsides.

7. Slow tempo bending
When lowering the flexion, it should be done in a controlled and slow manner, in order to emphasize the controlled work and motor control of the elbow. The ascent can be done more quickly, but not to the point of forcing the hyperextension of the elbow.
8. Flexion in rings
In this exercise, the rings are introduced to generate an external element of greater instability. Therefore, it should be done at a more advanced stage and when the pain is minimal, controlling the descent at all times and the movement so as not to destabilize the rings.
9. Isometric pull up
We will proceed to do a strict pull-up, being able to help ourselves with a jump at the time of making the ascent, and then perform an isometric at the top of the pull-up. This will make the elbow is controlling the position stabilizing the gesture well. It will begin with low times, increasing later, as the elbow will allow more tolerance to the exercise.

10. Eccentric pull up
As before, the first phase can be helped with a jump, but when performing the descent, the movement should be controlled for 2-3 seconds. In this exercise you must also have good scapular stability, otherwise, the work of the elbow will be excessive to control what should be controlling the shoulder.
To reduce inflammation and improve the recovery of irritated tissues, you can integrate red light therapy as additional support.
Conclusion
Although elbow injuries are not the most prevalent in CrossFit, it has been shown that they can be significant in an athlete's performance. As it may alter their training in weightlifting and gymnastic gestures. Most of these injuries can be related to overuse, motor control deficits and lack of stability in the area.
Prevention in these athletes will be based on an adequate progression to develop the necessary skills for the demands of this sport, with special emphasis on stability work, eccentric strength and motor control.
Once the pain is localized in the elbow and the cause of the pain is identified through an assessment by a healthcare professional, it can be addressed through education and an appropriate exercise approach. In addition to an adaptation of the training loads.






